This is online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent. Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs .This e-log book also reflects my patient centered online learning portfolio and your valuable comments on comment box is welcome.
I've been given this case to solve in an attempt to understand the topic of "patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations, and come up with a diagnosis and treatment plan.
17/6/23
Blog by Janhavi Virani
CHEIF COMPLAINTS:
A 45 year old male pt who is a Toddy collector by occupation resident of Nalgonda came to medicine opd with complaints of
1. Fever since 10 days
2. Decreased urine output since 10 days
3. B/L pedal Edema since 10 days
HISTORY OF PRESENTING ILLNESS:
Pt was apparently asymptomatic 10 years back then while climbing a palm tree pt developed dragging sensation of Right upper limb and lower limb put he continued his work , climbed down the tree and took rest . Upon waking up pt noticed he was not able to lift his right upper limb and lower limb with slurring of speech and deviation of mouth to the right side ,
Now 10 days ago , he developed B/L pitting type of Edema extending up to the knees .
Not associated with chest pain , palpitations, SOB .
Then he developed fever which is intermittent in nature , low grade not associated with chills and rigors , cough , cold , burning micturition, pain abdomen , vomitings , loose stools .
Since 10 days back pt also has complaints of decreased urine output not associated with dribbling, hesitancy, urgency .
PAST HISTORY:
Pt is a k/c/o CVA - 10 years back I.e right sided hemiparesis and is on Herbal Medication
K/c/o HTN since 10 years
Not a k/c/o DM, CAD , CAD , Thyroid disorders, Epilepsy, TB , Asthma
PERSONAL HISTORY:
Diet - mixed
Appetites - normal
Sleep - adequate
Bowel and bladder - regular ( decreased urine output)
Addictions- alcoholic ( Toddy drinker ) stopped 10 years back
FAMILY HISTORY:
No significant family history
GENERAL EXAMINATION:
Pt is conscious , coherent and cooperative
Moderately built and nourished
No pallor , icterus , clubbing , cyanosis, lymphadenopathy
Bilateral pedal Edema is present since 10 days ( extending uptil knee)
VITALS:
BP - 120/60mmHg
PR - 90bpm
RR - 18cpm
Temp - 97.8F
Spo2- 98% on RA
GRBS- 97 mg/dl
SYSTEMIC EXAMINATION:
CVS :
Inspection - percordium is normal
Position of trachea is central
No visible scars , sinuses , pulsations
No dilated or engorged veins
Palpation -no local rise of temperature , no tenderness
position of trachea is central
Apex beat at 5th intercostal space midclavicular line
No palpable thrills or heave
JVP not raised
Auscultation- S1 S2 heard , no murmurs
RESPIRATORY SYSTEM:
Inspection:-
oral cavity- Normal ,nose- normal ,pharynx-normal
Shape of chest - normal
Chest movements : bilaterally symmetrically
Trachea is central in position.
Palpation:-
All inspiratory findings are confirmed
Chest movements bilaterally symmetrical
AUSCULTATION
BAE+, NVBS
PER ABDOMINAL:
Soft , non tender
No organomegally
Bowel sounds heard
CNS:-
HMF-
Pt is conscious
Speech- slurred
Right Left
Spinothalmic
1. Crude touch- + +
2. Pain- + +
3.Temperature- + +
Posterior Coloumn
1. Fine touch + +
2.Vibration Felt Felt
( over bony prominence )
MOTOR EXAMINATION
Tone
UL- Hypo N
LL- Hypo N
Power
UL- 0/5 2/5
LL- 4/5 4/5
Reflexs
B +2 +1
T +2 +1
S +2 +1
K +1 +1
A - -
Plantars Extensor Flexor
PROVISIONAL DIAGNOSIS:
?AKI ?CKD
INVESTIGATIONS:
LIVER FUNCTION TEST (LFT)
Total Bilurubin Result 0.86
Direct Bilurubin 0.14
SGOT(AST). 32
SGPT(ALT). 27
ALKALINE PHOSPHATE 100
TOTAL PROTEINS #6.3
ALBUMIN. 4.1
A/G ratio 1.94
SERUM ELECTROLYTES
SODIUM. 141Units mEg/L
POTASSIUM. 3.5mEGIL
CHLORIDE. 99mEg/L
CALCIUM IONIZED 1.12
Serum Creatinine. 1.1mg/dl
RBS. #83mg/dl.
Blood Urea. 21mg/dl
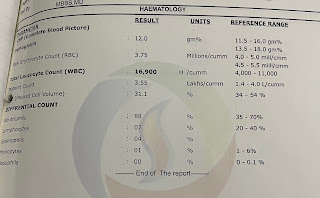
HEMOGRAM
HAEMO GLOBIN #12.0
TOTAL COUNT 5,650
NEUTROPHILS 57
LYMPHOCYTES. 32
EOSINOPHILS. 01
MONOCYTES. 10
BASOPHILS. 00
PCV. #36.6
M CV. 88.2
MC H. 29
MCHC. 32.8
POW-CY. 13.8
ROW-SD. 46.1
RBC COUNT. # 4.15
COMPLETE URINE EXAMINATION
APPEARANCE. Pale yellow
REACTION. Clear
SP.GRAVITY. 1.010
ALBUMIN. Nil
SUGAR. Nil
BILE SALTS. Nil
BILE PIGMENTS. Nil
PUS CELLS. 2-3
EPITHELIAL CELLS. 2-3
RED BLOOD CELLS. Nil
CRYSTALS. Nil
CASTS. Nil
AMORPHOUS. Absent
DEPOSITS
OTHERS. Nil
ECG-
2D ECHO
TREATMENT:
1. ECOSPRIN PO/HS
2. DOLO 650 mg PO/SOS







Comments
Post a Comment