1801006056 - LONG CASE
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent.
This is an online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan
Blog by Janhavi Virani
1801006056
A 34 year old female patient who is a farmer by occupation and is resident of choutuppal came to opd with chief complaints of -
1. Vomitings since 3 days
2. Abdominal pain since 3 days
HISTORY OF PRESENTING ILLNESS -
Patient complains of vomiting since 3 days which contains food particles ( occurring after intake of food ) 3-4 episodes in a day , yellowish in colour non projectile and non bloodstained .
History of abdominal pain since 3 days which she describes as diffuse and intermittent associated with nausea , throbbing type aggravated with eating.
Along with vomiting and abdominal pain patient also has generalised weakness affecting her daily activities.
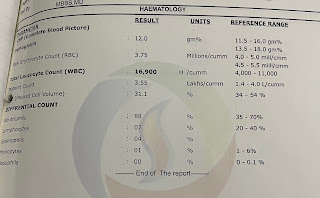
Patient was apparently asymptomatic 1 month back then she developed fever which was sudden in onset associated with chills and rigor , she also had 2-3 episodes of vomiting with pain in abdomen and watery , small volume, non blood stained loose stools . After which patient went to hospital and was diagnosed with anemia with Hb of 5.2gm% . She was advised admission in the hospital to which she refused and was started on oral iron therapy. She also ate iron rich food at home .
No history of burning micturition, urgency , increased frequency, Dyspnea , paroxysmal nocturnal dyspnea or any bleeding manifestations.
DAILY ROUTINE-
Patient wakes up at 6 am and does her daily morning activities then she has her breakfast at 9 am . She packs her lunch and leaves for work ( farmer ) where she has her lunch at 1 pm . She comes back home by 6 in the evening and does household chores has her dinner at 8 pm and sleeps by 9 pm .
Now because of weakness she is unable to do her daily work .
MENSTRUAL HISTORY-
Menarche at the age of 14 years
Cycles - 5/30 regular ( delayed by 5 days )
Usage of cloth
Associated with dysmenorrhea and presence of clots .
MARITAL HISTORY -
She was married at the age of 16 years
Non consanguineous marriage.
OBSTETRIC HISTORY-
She has 2 kinds
LSCS w as done in both the pregnancies. While 2nd pregnancy patient has history of blood transfusion .
PAST HISTORY-
No similar complaints in past
Patient is not a known case of Diabetes Mellitus , Hypertension, Epilepsy, CAD or any thyroid abnormality.
DRUG HISTORY-
Intake of 1. Iron and folic acid tablets since 1 month
2. Omeprazole and Domperidone tablets
3. Sefexim 200 mg tablet
4. Vitamin supplements

FAMILY HISTORY-
No significant family history
PERSONAL HISTORY-
Diet - mixed
Appetite - normal
Bowel and bladder- regular
Sleep - adequate
No addictions
GENERAL EXAMINATION-
Patient is conscious coherent and cooperative
Moderately built and nourished
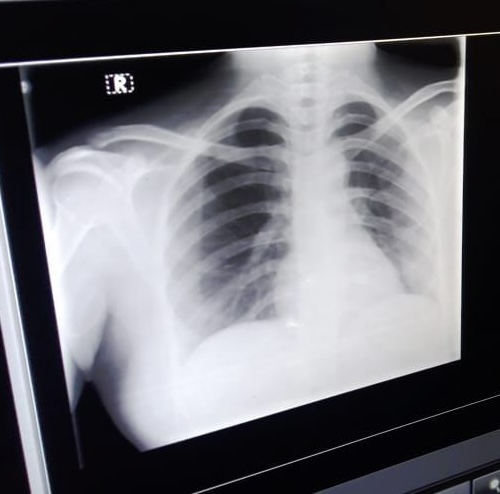
Pallor- ++






VITALS -
Temperature- a febrile
BP - 110/70 mm of hg
Pulse rate - 65 bpm
Respiratory rate - 17 cpm

SYSTEMIC EXAMINATION-
ABDOMEN EXAMINATION-
INSPECTION-
Shape - round large with no distension
Umbilicus - inverted
Equal symmetrical movements in all quadrants with respiration
No visible pulsations , palpations , dilated veins or localised swelling
LSCS scar present in lower abdomen, hyperpigmented
Hernial orifices are free
PALPITATION -
No local rise of temperature
Diffuse tenderness ( present in left lumbar , umbilical, hypo gastric areas)
Deep palpitations-
No organometaly
PERCUSSION- liver dullness heard at 5th intercostal space
AUSCULTATION-
Bowel sounds present
No bruit heard
Cardiovascular system-
Respiratory System-



IV fluids ns 75ml/hr
INJ pan 40 mg/ IV /od
INJ Zofer 4mg/IV
INJ optineuron 1 amp in 500ml ns/ IV/od
T.PCM 650 mg od
Syp.Sucralfate 10ml/tid
Syp. Cremaffin citrate 15ml
INJ vitkofol 1000mcg/IM/od
T.orofer xt/po/od

Comments
Post a Comment